Answer the Following Questions Accurately to Authorize Your Application!
Step
1
of
4
25%
Name
(Required)
First
Last
Phone
(Required)
Email
(Required)
Gender
(Required)
Male
Female
Address
(Required)
Street Address
Address Line 2
Alabama
Alaska
American Samoa
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Guam
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Northern Mariana Islands
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
U.S. Virgin Islands
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
Armed Forces Americas
Armed Forces Europe
Armed Forces Pacific
State
ZIP Code
Primary Date Of Birth
(Required)
Month
Day
Year
Social Security Number
(Required)
Please Enter Your 9 Digit SSN NUMBER
Do You Have A Spouse To Enroll? *
(Required)
YES
NO
Full name Of Spouse
(Required)
Date of Birth
(Required)
Month
Day
Year
Social Security Number
(Required)
Terms and Condition
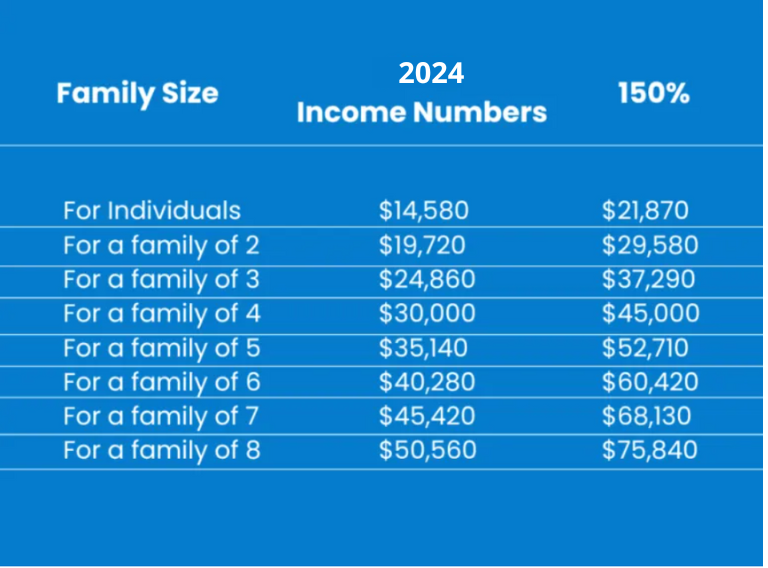
I give my permission to Insurance Plans of America, Latonya Meriwether and Jayla Burgess to serve as the health insurance agents or brokers for myself and my entire household, if applicable, for purposes of enrollment in a Qualified Health Plan offered on the Federally Facilitated Marketplace. By consenting to this agreement, I authorize the above-mentioned agents to view and use the confidential information provided by me in writing, electronically, or by telephone only for the purposes of one or more of the following. Searching for an existing Marketplace application. Completing an application for eligibility and enrollment in a Marketplace Qualified Health Plan or other government insurance affordability programs, such as Medicaid and CHIP or advance tax credits to help pay for Marketplace premiums. Providing ongoing account maintenance and enrollment assistance, as necessary; or responding to inquiries from the Marketplace regarding my Marketplace application for the next 60 months. I understand that the agents will not use or share my personally identifiable information (PII) for any purposes other than those listed above. The agents will ensure that my PII is kept private and safe when collecting, storing, and using my PII for the stated purposes above. I confirm that the information I provided the agents and the information used on my application is true and accurate. I understand that I do not have to share additional personal information about myself or my health with my agents beyond what is required on the application for eligibility and enrollment purposes. I understand that my consent remains in effect until I revoke it, and I may revoke or modify my consent at any time by contacting my agents at the following email info@insuranceplansofamerica.com Name of Primary Writing Agent: Latonya Meriwether. Phone Number: 1-877-752-6711. Email Address: info@insuranceplansofamerica.com Agent NPN: 9690699. By submitting this document, you agree the above information is true and accurate. Also that your income falls in the following chart, qualifying you for the Zero Premium or Subsidized Health Coverage.
Date Of Apply
(Required)
Month
Day
Year
Signature
(Required)
Skip to content
Open toolbar
Accessibility Tools
Accessibility Tools
Increase Text
Increase Text
Decrease Text
Decrease Text
Grayscale
Grayscale
High Contrast
High Contrast
Negative Contrast
Negative Contrast
Light Background
Light Background
Links Underline
Links Underline
Readable Font
Readable Font
Reset
Reset